


The following is a Guest Article by Doc Martyn. Opinions and statements within are his own. Originally published by him on the 6th of May, 2023
- Paul, of Buriram Expat Food and Drink, asked me to see his 53-year-old partner, Noi. She had suffered from Type 2 diabetes for 4 years; she had been generally unwell for the last couple.
- The following is a transcript of the medical notes I made during the consultation:
Past Medical History: Appendicectomy, TB 6 years ago, Type 2 diabetes (aka NIDDM; Non-Insulin Dependent Diabetes Mellitus). Alcohol abuse.
Family History: Father and brother died from alcohol abuse, smoking.
Social History: De-facto relationship, works in retail, alcohol 10gm/day, no tobacco, or illicit drug use.
Medication: Glipizide 5mg 1 am, Metformin 500mg 1 pm.
Presenting complaint: Paraesthesia palms and soles of feet, not stocking distribution (usually found in Diabetic Neuropathy). Frequent urination with nocturia +/- dysuria, (painful urination) and vulval itch.
Examination: Height 165cm, Weight 48Kg, BP 119/73, Pulse 89SR (Normal Sinus Rhythm), Oxygen saturation 98% (normal).
Urinalysis glucose++++, ketones +
Heart and lungs normal.
Abdominal examination; liver smooth, soft, and non-tender, but slightly enlarged.
Early Dupuytren’s Contractures (DCs) both hands, see photos 1 and 2. DCs are typically found in Caucasians especially males over the age of 50. Examples include; the UK actors Bill Nighy and David McCallum, Ronald Reagan, and Margaret Thatcher. This pathology is uncommon in Asians, especially Asian females. The cause of DC is not clear, but there appears to be a genetic predisposition. Risk factors for DCs include; alcohol abuse, thyroid disease, liver disease, and diabetes.


Diagnosis:
-Poorly controlled Type 2 Diabetes.
-No significant diabetic neuropathy.
-Hepatomegaly/hepatitis.
-Dupuytren’s Contractures
Management:
-Medication; her medication dose was woefully inadequate. The Glipizide was ceased. The Metformin 500mg was increased to 1 three times /day.
-She was advised to immediately cease eating all carbohydrates, including sugar.
-The following pathology tests were ordered: CBC, HbA1c, Liver function tests (LFTs), Thyroid Stimulating Hormone (TSH), Vit B12, LDL cholesterol, and triglycerides
- The results:
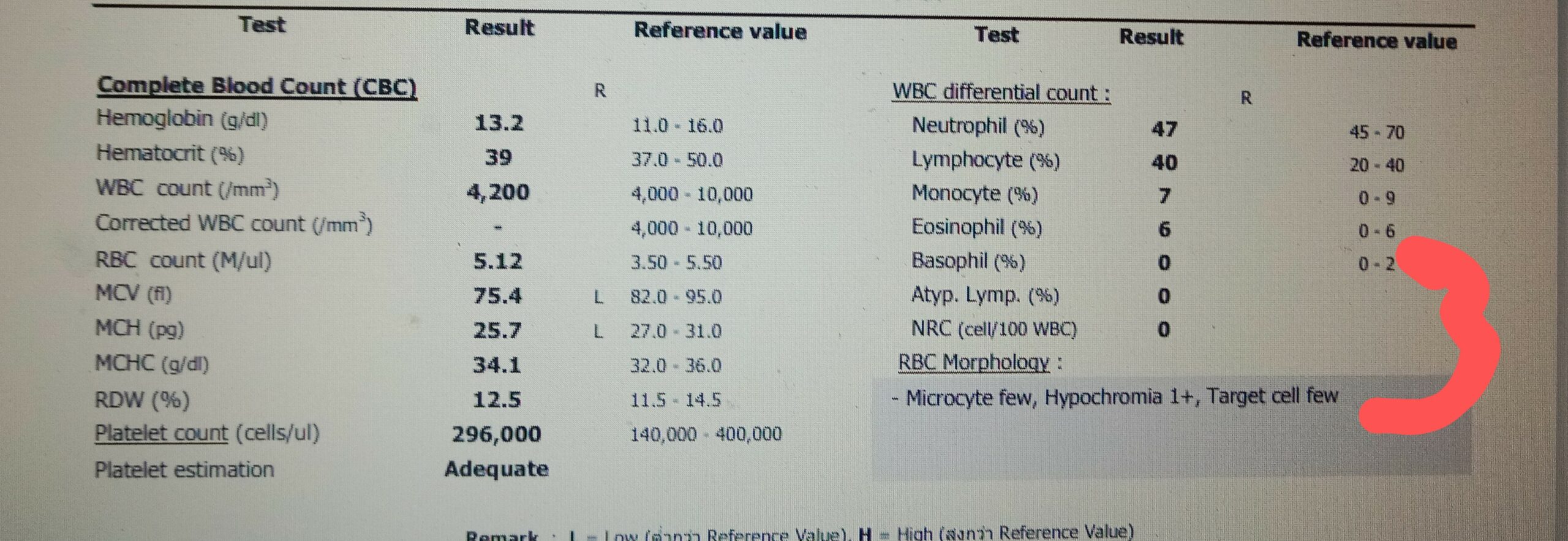
-Her complete blood count was within normal limits, see photo 3.
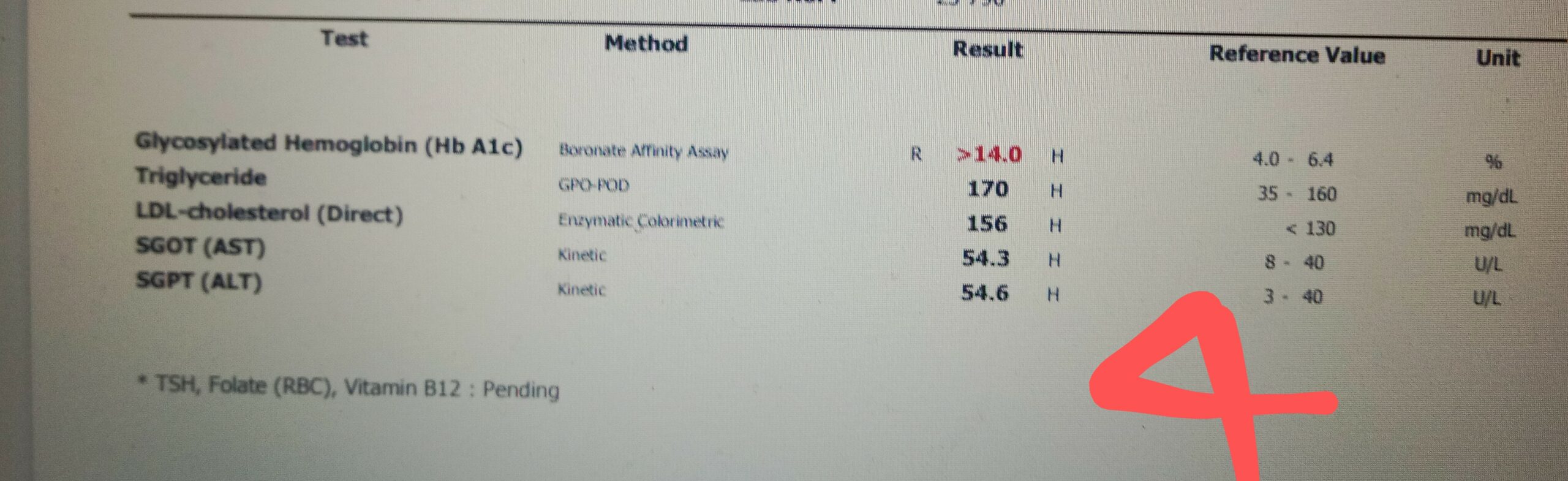
-Her HbA1c was exceptionally high, see photo 4. What is HbA1c? The hemoglobin in human red cells combines with the glucose in the bloodstream, to become glycated haemoglobin. If the glucose level in the blood is high the level of glycated haemoglobin in the red cells, the HbA1c, increases. In general, red cells last 120 days. The HbA1c is therefore a measure of the patient’s average glucose level over the preceding 3 months. In Noi’s case, her level had been ‘off the chart’ for at least 3 months. It was impossible to know how long her HbA1c had been so high.
This is serious: Prolonged hyperglycaemia, diabetes, damages the blood vessels resulting in eye damage and blindness, kidney damage and renal failure, coronary artery disease and heart attack, and peripheral vascular disease and amputation. It also causes neuropathy, and nerve damage.
-Her LDLs 156 (significantly elevated), Triglycerides 170 (elevated), see photo 4, increasing her risk of heart disease.
-Her LFTs were abnormal, see photo 4, confirming hepatitis.
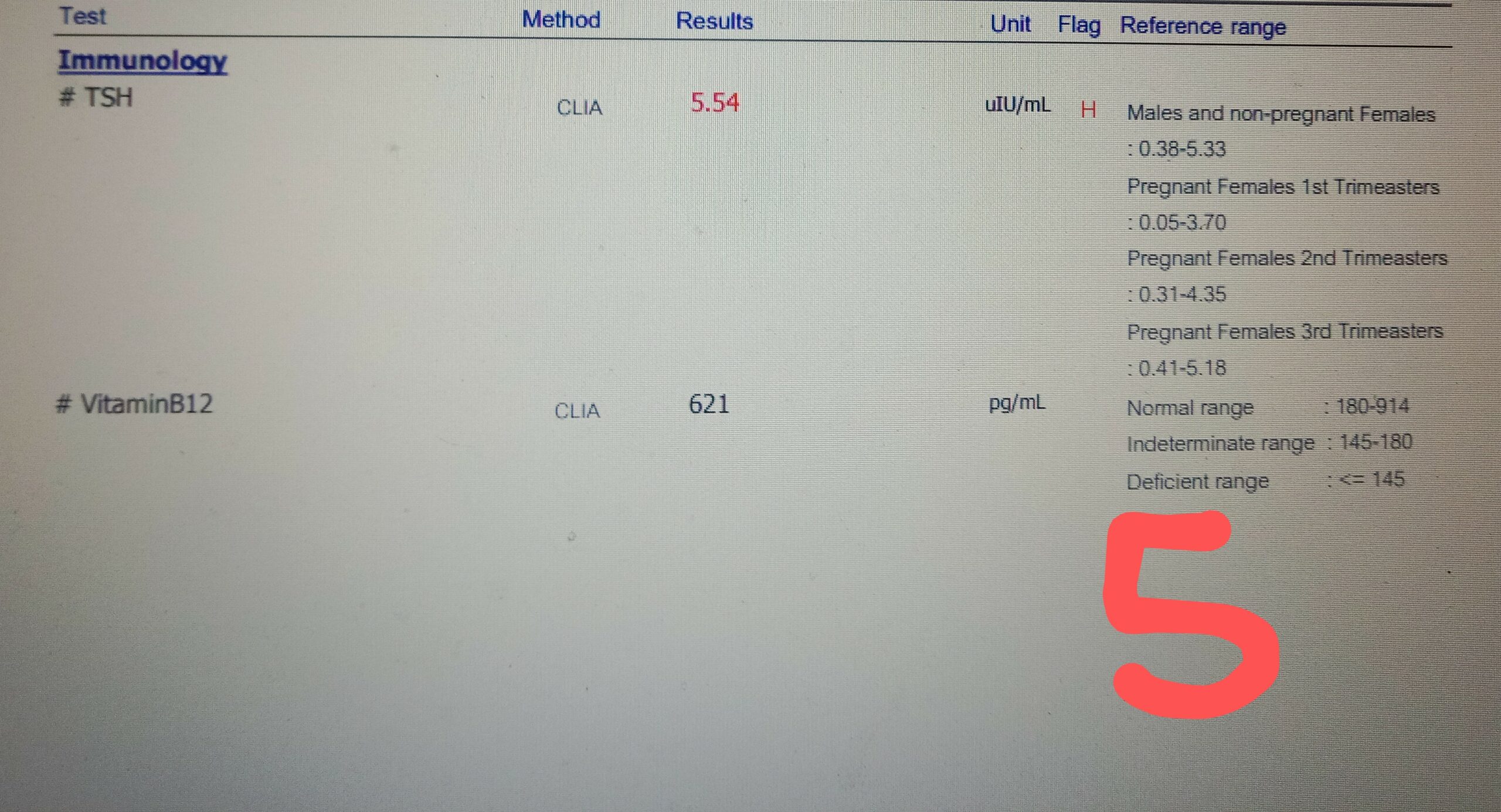
-Her TSH was elevated, she was hypothyroid, and her thyroid was underactive, see photo 5.
-Her B12 was normal, see photo 5.
- Noi was very unwell; indeed, she was a ticking time bomb. Considering all the results, her therapy was altered. Her Metformin was increased to 5 tablets/day, the maximum dose. Thyroxine 100mcg alternate days was added, Thyroxine replacement therapy takes about 6 weeks to be fully effective.
Normal fasting BSL in a non-diabetic range between 3.9-5.6 mmol/l. The following is the list of Noi’s weekly average morning fasting blood sugar levels since therapy was altered:
Week 2: 17.3, Week 3: 14.7, Week 4: 12.4, Week 5: 7.3, Week 6: 6.75. This is an encouraging outcome.
- Review haematology will be performed next week to assess her thyroid function and her liver function. Her cholesterol levels will be reviewed 2 months after her fasting BSL remains within normal limits.
- Glucose in the blood provides the cells of the body with energy, akin to petrol in an ICE. Insulin is the hormone that facilitates the absorption of the glucose into the cells. Type 1 diabetes results from pancreatic failure, caused by an autoimmune disease that destroys the Beta cells of the pancreas, the cells which release insulin. Type 2 diabetes is caused by insulin resistance, normally due to obesity. Obesity is a Western epidemic caused by gluttony and a poor diet, see photo 6. In the decade from 2011 to 2021, the USA diabetic rate increased from 9.8% to 11%. Over the same period, Thailand’s diabetic rate increased from 7.5% to 10%!

- There is an ever-increasing abundance of obese Thais, particularly Thai children. A significant cause of this is the inclusion of harmful Western processed foods in their diet. But this is not the only cause. Recent research indicates the increase is also caused by the interaction of three different factors:
-Genetic variants: Asians have variants in the genes required for normal Beta cell function, which causes a reduction in insulin supplied by the Beta cells. And mutations of their gene GRB14; result in increased insulin resistance.
-Physiological adaptation: As a result of the nutritional privation caused by multiple famines over the millennia, Asians have developed a starvation adaptation; which increases their ability to efficiently process food and store fat to provide advantage during famine.
-Culture: Big dinners are not only a means to communicate and support the community, they are also used to celebrate and honor the ancestors. These meals were predominantly rice-based and, despite the introduction of Western cuisine, they still are.
These factors have resulted in a Thai population that is poorly conditioned for modern-day Western style indulgent gastronomic gratification.
The answer; as in Noi’s case, arrest the Thai’s dependence on carbohydrates, in particular rice, sweet desserts, sugar, and sugary drinks, and/or discourage the inclusion of Western cuisine.
- Worldwide, in 2019, 463 million people between the ages of 20 and 79 suffered from diabetes. This represents 9.3% of the world population in this age group.
Individuals with diabetes have a 2–3 fold increased risk of all-cause mortality.
The rate of Type 2 diabetes in Thailand continues to increase and it is expected to exceed the diabetes rate in the USA by 2025.
Diabetes is a complex illness that requires regular, at least 6 monthly, medical assessments. Yet, in Thailand, such care is not readily available through the public health care system, which has limited resources. And, as patient numbers increase over the years, the limited resources will be stretched even further.
I have walked through and managed patients in the Orthopaedic Intensive Care department in the new wing of the Buriram Public Hospital. Thais do not deserve to have their limbs amputated, see photo 7 below (Warning, Graphic), because of inadequate medical management of their Diabetes, “The scourge of Thailand”.


{kind=link}